Patients Demonstrate Hand Restraints, 1915, courtesy The Burns Archive
The Indian Office provided rules for attendants working at the Canton Asylum for Insane Indians which were thorough and explicit; similar instructions were most likely the case in all other insane asylums. Patients were supposed to “preserve order” but only by using the mildest means possible. Rule 20 stated: “No kicking, striking, shaking, or choking of a patient will be permitted under any circumstances. Patients must not be thrown violently to the floor in controlling them, but the attendant shall call such assistance as will enable him to control the patient without injury.”
This rule was broken any number of times, and at least one male attendant was fired for committing unwarranted violence against patients. Mechanical restraints like cuffs and camisoles (straitjacket) were to be used only with the consent of the physician or superintendent, but employees did not follow this rule. Instead, they got restraints from the financial clerk simply by asking for them. Dr. Hummer, who later received very harsh criticism for the asylum’s excessive use of restraints, either permitted their use (though he often said restraints weren’t used) or he abdicated his responsibilities to the financial clerk. Either way, he had to know that employees were using restraints quite freely . . . unless he wasn’t making rounds often enough to catch it. Whatever the reason for all the restraints, Dr. Hummer was responsible for the situation.
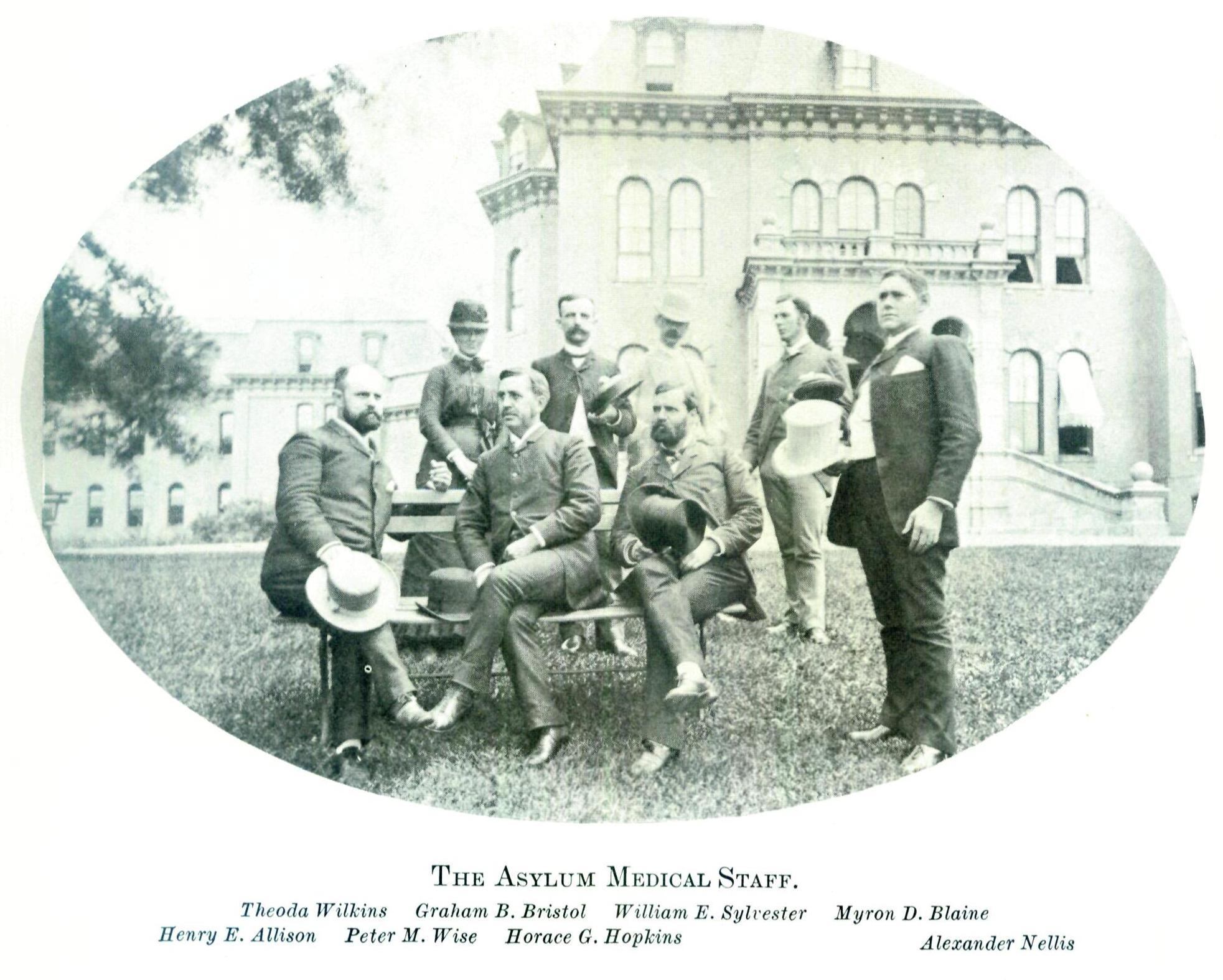
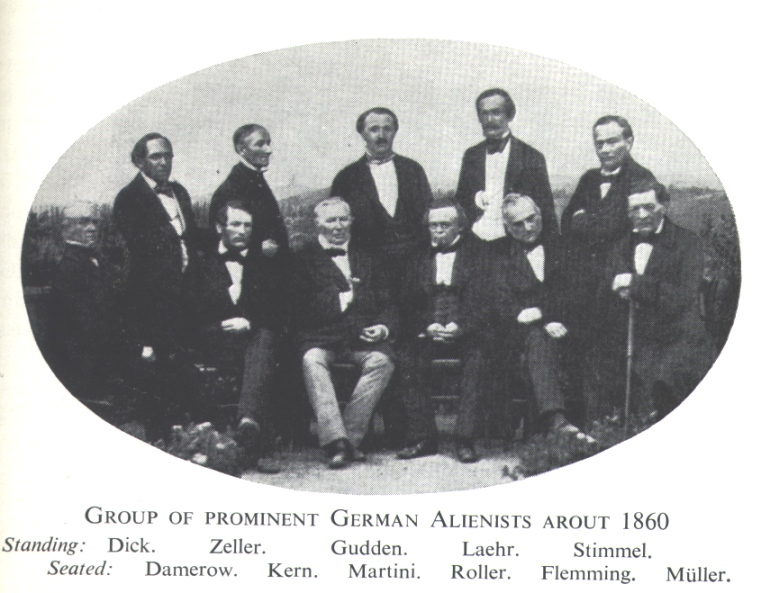
Medical Staff at Willard Asylum

Staff of Arizona State Asylum, 1914