
Corn Dance, Taos Pueblo, circa 1920s
Though the majority of the U.S. population celebrates an official day of gratitude called Thanksgiving, Native Americans have always had a deep tradition of routinely giving thanks. They have particularly given attention and gratitude to the animals and plants which gave their lives to provide sustenance or medicine.
Planting ceremonies were also important, as were dances and feasts to celebrate good crops. Among others, the Creek, Cherokee, Seminole, Yuchi, and Iroquois tribes celebrated the Green Corn Festival, which marked the beginning of the first corn harvest. It was a time to thank Mother Earth and all living things for providing food and other usable items that made life good. The Maple Syrup Ceremony (late spring), Strawberry Ceremony (early summer), Bean Dance and Buffalo Dance (winter), are only a few of the times that Native Americans set aside to acknowledge their dependence upon the bounty of the earth.

Buffalo Dance at Hano, courtesy www.firstpeoples.us
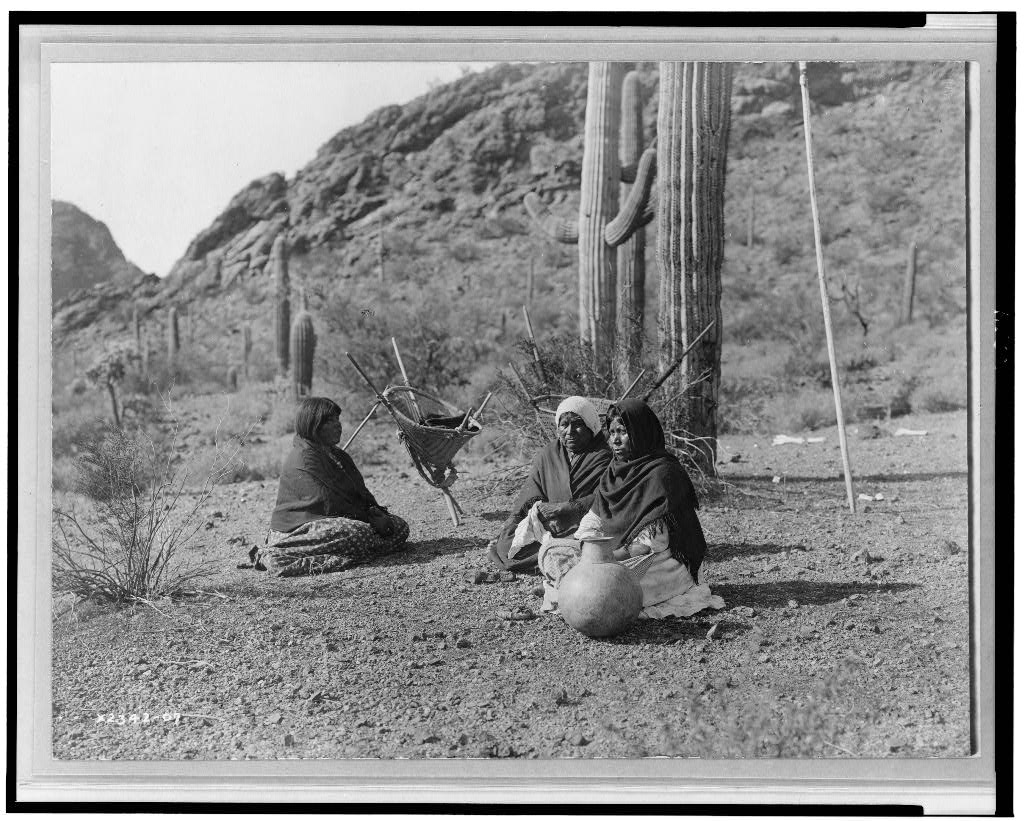
Qahatika Women Resting in Harvest Field, courtesy Library of Congress
The Iroquois particularly formalized times of thanksgiving, which would include a special Thanksgiving Address. A speaker was chosen to give thanks on behalf of all the people. The thanksgiving prayer then offered gratitude to the Creator for the earth and the living things upon it. The prayer could be quite long, encompassing specific things the speaker wanted to call special attention to, like birds, rivers, medicinal grasses and herbs, wind, rain, sunshine, the moon and stars, and so on. Thanksgiving festivals provided opportunities to feast, express gratitude, and enjoy good things, and also provided times of cleansing, healing, forgiveness, and reconciliation.

























