Dedicated Alienists Tried to Stay Informed
One of the major problems with the Canton Asylum for Insane Indians was that commitment rules were so lax. Like most asylums, there were patients incarcerated because they were inconvenient to others or created problems for civil authorities, but there were also some patients who genuinely needed help. In either case, few patients admitted to the asylum had actually been evaluated by a physician of any kind, let alone one who specialized in mental illness. Instead, they were usually sent to the asylum on the assessment of only a layperson (Indian agent or reservation superintendent) which was terribly unfair. Abuses of power could, and did, take place, because even if these lay persons were actually trying to help someone, they weren’t necessarily right in their opinion of the person’s mental state.
Though abuses of power probably occurred everywhere at times, patients in other states and institutions often had stronger protections. Massachusetts had always been a progressive state when it came to helping its citizens facing mental health issues, and its commitment laws were fairly strict. In 1916, the editors of Institutional Care of the Insane in the United States and Canada wrote: “Commitment [in Massachusetts] may not be made unless there has been filed with the proper judge or justice a certificate of the insanity of the person by two physicians nor without an order signed by the proper judge that he finds the person insane.”
The judge could see and examine the person if he thought it needful, could also call in a third physician, and could summon a jury of six men to hear and judge whether the proposed patient was insane or not. Furthermore: “A physician making a certificate of insanity must be a graduate of a legally chartered medical school, in actual practice for three years and for the three years last preceding, and be registered. His standing, character and professional knowledge of insanity must be satisfactory to the judge.”
Though there could certainly be an “old boy” system that would allow a motivated complainant the opportunity to have a family member or enemy committed to an insane asylum, it was still much more difficult for two physicians and a judge to collude against a person than it was for one layperson to decide that an Indian was crazy.
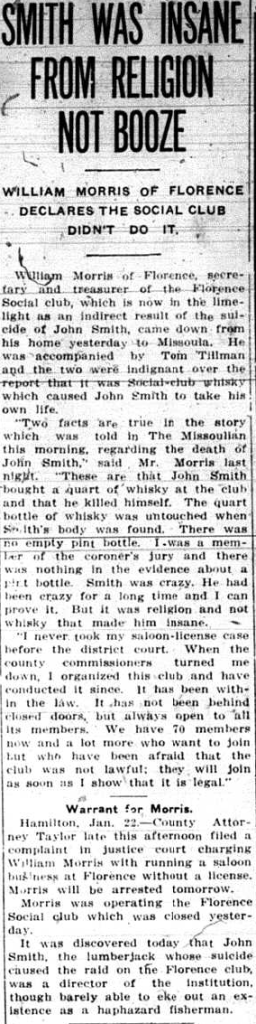
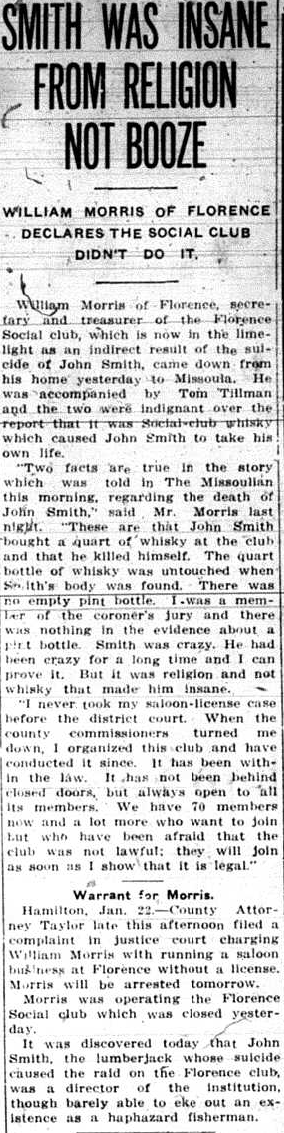
Newspaper Story Argued Whether Man Was Insane From Booze or Religion

Danvers State Hospital, circa 1893